Photo by National Cancer Institute on Unsplash
Mark Shrime, RCSI University of Medicine and Health Sciences
Dr John Baptist Mukasa, or JB Neuro, as his colleagues called him, “was always at the beck and call of everyone who needed neurosurgical care”, according to his colleague Dr Sabrina Kitaka. Mukasa’s death from COVID on June 29, in the middle of Uganda’s most lethal wave so far, robbed the country’s medical fellowship of a friend and a mentor.
It also cut the total number of neurosurgeons in Uganda by 25%.
Only three neurosurgeons remain in Uganda, a country of 44 million people (although some estimates put the workforce as high as ten). By comparison, Canada, with a population of 35 million, has over 150 neurosurgeons. New York City’s Columbia Presbyterian Hospital, where I did my residency, has 17 neurosurgeons in one department alone – several times larger than the entire neurosurgical workforce of Uganda.
There are many reasons for this disparity, including a lack of training facilities and hospitals capable of supporting complex surgical care. And then there’s the brain drain – the migration of trained professionals out of a country to other, often wealthier, locations.
There are many reasons doctors leave. A higher salary, access to education, stable political conditions, improved standards of living, increased perceived quality of life, and greater personal safety all draw doctors away from their homes and often to countries that previously colonised theirs.
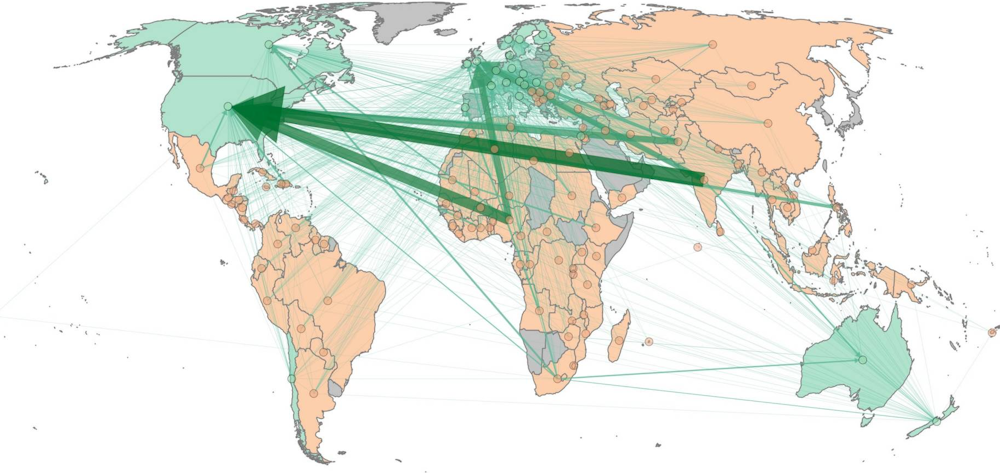
It’s a multi-billion–dollar industry. Recently, my colleagues and I published an estimate of the economic effect of the migration of doctors (we didn’t have enough information to look at the migration of nurses or other health professionals). We found that countries lose somewhere between US$3.5 billion and US$38 billion a year as a result of the excess deaths that brain drain causes. The countries exporting the greatest number of doctors incur the largest costs: India, Nigeria, Pakistan and South Africa.
In other words, not only do the countries to which doctors migrate benefit from an influx of trained, experienced professionals, they also inflict what is essentially a tax on the economies of source countries — all for the privilege of attracting away their clinical staff.
In 2010, the World Health Organization agreed the Global Code of Practice on the International Recruitment of Health Personnel. This agreement encouraged source countries to hold onto their healthcare workforce by improving education, living standards and working conditions (it didn’t address how this could be achieved in the face of limited resources). The agreement also required destination countries to stop recruiting from countries with a shortage of healthcare workers.
But that never happened. In fact, at the beginning of the COVID pandemic, active recruitment of doctors from these source countries stepped up as the scale of the crisis became clear.
COVID initially hit richer countries in Europe and the US hard, pummelling Italy, Spain and New York City, leaving countries in Africa relatively unscathed. It seemed pretty miraculous, prompting commentators to offer reasons for Africa’s relative success.
Calls rose for medical professionals from resource-constrained regions to help shoulder the burden of the pandemic in these wealthier countries — flying in the face of the WHO code of practice. These calls went beyond simple recruitment. Some offered additional incentives to entice doctors to stay: for example, the UK fast tracked registration of doctors trained outside the country.
Now that the pandemic has swung back to ravage Africa, India and other parts of the world, this is a favour that the more wealthy nations have not returned.
Since I began writing this piece, Uganda also lost a 36-year-old ENT surgeon, Dr Ian Bwete Apuuli. During the pandemic, he performed tracheotomies on COVID patients, allowing them the chance to breathe without ventilation. But tracheotomies generate aerosols, and aerosols carry infection. Apuuli succumbed to the disease, leaving Uganda with only one surgeon trained to remove tumours from the head and neck.
The brain drain of healthcare workers from countries that can scarcely afford to lose them is not an emotionless, economic discussion. When we actively entice doctors not just to come and help, but to and come and stay, the effect is more than temporary. It is more than monetary. It undermines the entire health systems of the countries these doctors leave behind.
Mark Shrime, Chair of Global Surgery, RCSI University of Medicine and Health Sciences
This article is republished from The Conversation under a Creative Commons license. Read the original article.
{kind=link}